Musculoskeletal dysplasias – comprehensive diagnosis and treatment
Help your child regain normal development and full mobility through comprehensive care provided by the specialists at the Paley European Institute, world leaders in the treatment of congenital musculoskeletal disorders.
The key to success is early diagnosis and immediate treatment.
What are musculoskeletal dysplasias?
Musculoskeletal dysplasias are a group of congenital developmental disorders of the musculoskeletal system that affect the growth and structure of bones, cartilage, and connective tissues. They are characterized by disproportionate growth of body parts, abnormalities in the development of long bones, structural abnormalities of the spine, and joint dysfunction.
The severity of symptoms can range from mild to severe, requiring a multidisciplinary approach. Early diagnosis and comprehensive treatment are essential to ensuring the best possible quality of life for patients.
Musculoskeletal Dysplasias
Reasons
Musculoskeletal dysplasias are most often the result of genetic mutations that disrupt the normal formation and growth of bone and cartilage tissue. These mutations can be inherited from parents or arise spontaneously—de novo—without a prior family history.
The most commonly affected genes include FGFR3 (achondroplasia, hypoachondroplasia), COMP (pseudoachondroplasia), and SLC26A2 (dystrophic dysplasia). In some cases, such as Morquio syndrome, the cause is a metabolic disorder leading to the abnormal accumulation of substances in tissues.
Additional risk factors include abnormal fetal positioning in the uterus, low amniotic fluid levels, and a strong family history of the condition.
Symptoms
The symptoms of musculoskeletal dysplasia vary and depend on the specific diagnosis, but the most common include:
Short stature: disproportionate or proportionate shortening of the limbs and/or trunk
Limb deformities: valgus (bowlegs), varus (knock-knees), shortening, or curvature of the long bones
Spinal abnormalities: scoliosis, kyphosis, cervical instability
Joint dysfunction: hypermobility, contractures, or early-onset osteoarthritis
Musculoskeletal pain: particularly in the hips, knees, and spine
Mobility difficulties: gait disturbances, limited mobility
In newborns and infants, symptoms may be subtle or absent, which is why screening in the first weeks of life is so important. Some cases of dysplasia do not become apparent until between the ages of 1 and 3, as the child experiences rapid growth and increased physical activity.
Diagnostics
The diagnosis of musculoskeletal dysplasia requires a multidisciplinary approach and is based on several key principles:
Clinical examination: assessment of body proportions, range of motion in the joints, posture, and gait by an experienced orthopedic surgeon.
Imaging studies: X-rays of the long bones and spine reveal characteristic changes in the structure of the epiphyses, metaphyses, and bone shafts. Magnetic resonance imaging (MRI) allows for a precise assessment of articular cartilage and soft tissues.
Genetic testing: Identification of specific gene mutations allows for definitive confirmation of the diagnosis, assessment of the risk of inheritance, and treatment planning. Prenatal diagnosis is possible as early as the second trimester of pregnancy using ultrasound and amniotic fluid testing.
Metabolic testing: In the case of mucopolysaccharidoses (e.g., Morquio syndrome), measuring lysosomal enzyme activity is crucial.
ACHONDROPLASIA
The most common form of genetic dwarfism, caused by a mutation in the FGFR3 gene. It is characterized by short limbs with a normal-length trunk, an enlarged head with a distinctive forehead, increased lumbar lordosis, and possible spinal abnormalities and bowlegs.
Diagnostics: X-rays of the limbs and spine, genetic testing (FGFR3 mutation), prenatal testing (ultrasound + amniocentesis).
Indications for treatment: Surgical limb lengthening using the Ilizarov method, correction of limb deformities, treatment of spinal defects, spinal stenosis, and cervical spine instability. Comprehensive postoperative rehabilitation.

PSEUDOACHONDROPLASIA
A genetically determined skeletal dysplasia caused by a mutation in the COMP gene. Symptoms appear between the ages of 1 and 3—short stature with disproportionately short limbs, deformities of the long bones, excessive joint laxity, and early-onset osteoarthritis of the hips and knees.
Diagnosis: X-rays (shortening and deformities of long bones, irregular epiphyses), genetic testing (COMP mutation).
Indications for treatment: Corrective osteotomies of the lower limbs, limb lengthening using the Ilizarov or Precice method, hip and knee joint reconstruction procedures, and intensive rehabilitation.
HYPOCHONDROPLASIA
A milder form of skeletal dysplasia caused by a mutation in the FGFR3 gene. It is characterized by proportional shortening of the limbs and less severe short stature than in achondroplasia. Symptoms may be subtle and become apparent gradually as the child grows.
Diagnosis: X-rays (shortening of long bones—particularly the femur and humerus), genetic testing (FGFR3 mutation).
Indications for treatment: Surgical bone lengthening using the distraction osteogenesis method (Ilizarov, internal/external telescopic nails), rehabilitation and physical therapy, treatment of functional deformities.

SPONDYLOEPIPHYSEAL DYSPLASIA (SED)
A genetic disorder characterized by abnormal development of the epiphyses of long bones and the vertebral bodies. It leads to short stature, deformities of the spine and joints, pain, and limited mobility. Symptoms appear during childhood.
Diagnostics: X-rays and MRI (flattening of the epiphyses, changes in the vertebrae), genetic testing.
Indications for treatment: Treatment of limb and spinal deformities, corrective osteotomies, rehabilitation, and, where indicated, joint replacement surgery.
MULTIPLE EPIPHYSEAL DYSPLASIA (MED)
A genetic disorder characterized by abnormalities in the development of epiphyseal cartilage, leading to abnormal formation of long bones and joints. It primarily affects the hips, knees, ankles, and shoulders—causing pain, limited mobility, and bone and joint deformities.
Diagnostics: X-ray (flattening and fragmentation of the epiphyses), MRI (assessment of articular cartilage), genetic testing.
Indications for treatment: Physical therapy, orthoses, corrective osteotomies, joint surface reconstruction, and joint replacement in advanced cases.
STICKLER'S TEAM
A rare inherited connective tissue disorder caused by mutations in collagen genes (COL2A1, COL11A1, COL11A2). It affects the joints, vision, hearing, and the facial skeleton. The course is variable, often leading to early-onset osteoarthritis and ophthalmic complications (risk of retinal detachment).
Diagnostics: Clinical examination (joints, face, hearing, vision), X-rays and MRI, ophthalmological and audiological tests, genetic testing.
Indications for treatment: Correction of limb deformities, treatment of degenerative conditions, physical rehabilitation, and interdisciplinary ophthalmological and audiological care.
DIASTROPHIC DYSPLASIA (DTD)
A rare genetic disorder caused by a mutation in the SLC26A2 gene. It is characterized by short stature, joint deformities (clubfoot, "buttonhole" thumb contracture), auricular deformities, and scoliosis. It requires specialized orthopedic care from birth.
Diagnostics: Prenatal ultrasound, postnatal X-rays (shortened and thickened bones, joint and spinal deformities), genetic testing (SLC26A2 mutation).
Indications for treatment: Correction of clubfoot (Ponseti method or surgery), limb lengthening (PRECICE or external fixators), correction of knee deformities and contractures, spinal stabilization for scoliosis/kyphosis, orthotic devices, and physical therapy.
Treatment of Musculoskeletal Dysplasia at the Paley European Institute
Treatment for musculoskeletal dysplasia at the Paley European Institute is comprehensive and tailored to the individual needs of each patient.
Guided growth
During the growth phase, it is possible to precisely correct limb alignment using a minimally invasive technique called hemiepiphysiodesis. Small plates inserted through incisions of about 5 mm inhibit growth on one side of the bone, gradually correcting the deformity without the need to cut the bone. The correction process typically takes one to two years.
Limb lengthening
In cases of significant limb shortening, we use modern methods of distraction osteogenesis: the Ilizarov method and the PRECICE system (a telescopic nail inserted into the bone), which ensures comfort and discretion during treatment.
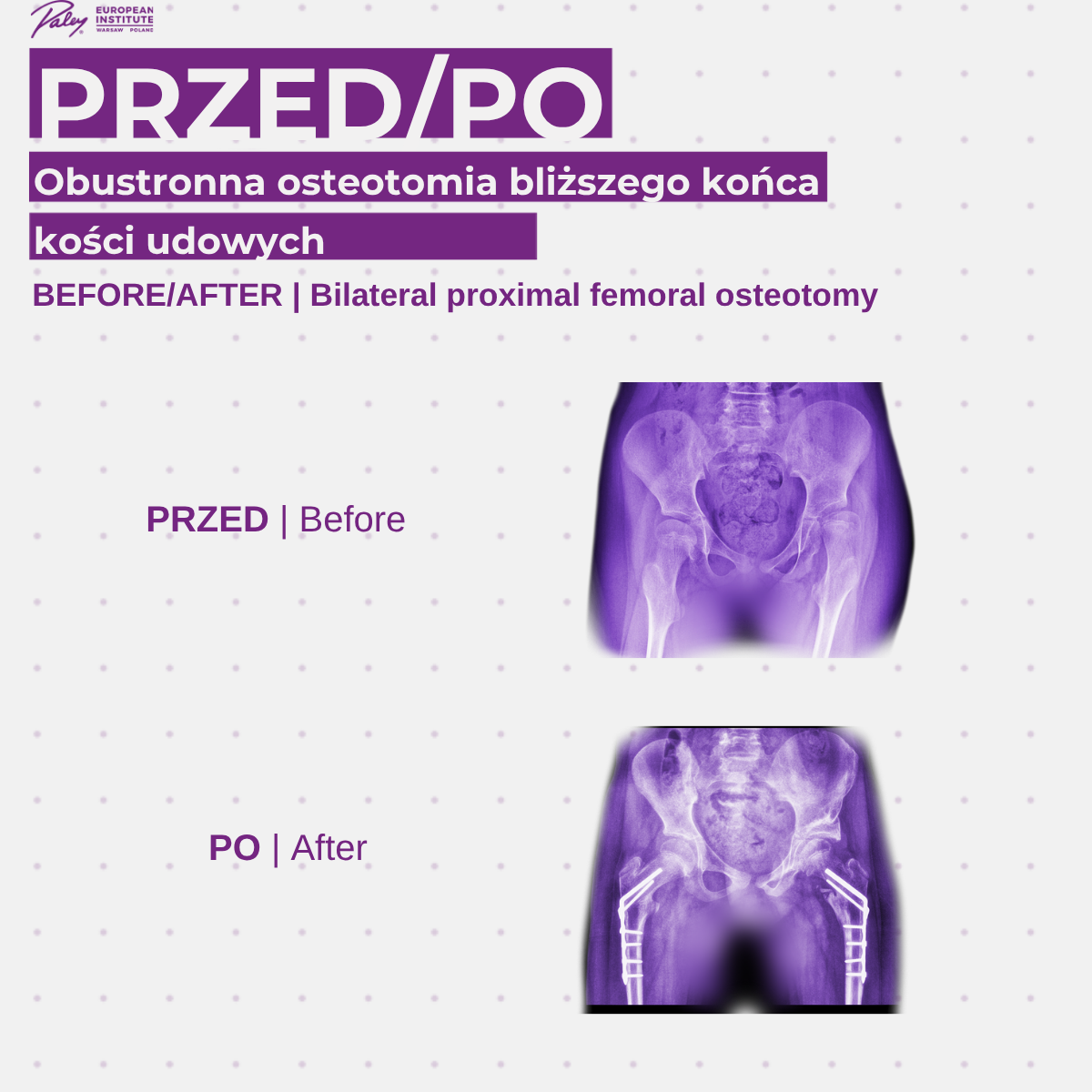
Corrective osteotomies
Surgical bone realignment in cases where guided growth is no longer possible or the deformity is too advanced.
Spinal stabilization
It includes the treatment of scoliosis, kyphosis, and cervical instability, which can threaten the spinal cord.
Rehabilitation and physiotherapy
An integral part of every stage of treatment. It includes exercises to strengthen muscles, improve range of motion, and teach proper gait patterns.
Orthotic supplies
Custom-fitted braces and supports designed to assist the function of the limbs and spine.
Multimedia
Your most frequently asked questions
What You Need to Know About Musculoskeletal Dysplasias
Musculoskeletal dysplasias are a group of congenital developmental disorders of the musculoskeletal system that affect the growth and structure of bones, cartilage, and connective tissues. In most cases, they have a genetic basis; they may be inherited from parents or result from a new, spontaneous mutation.
Symptoms vary depending on the type of dysplasia. The most common symptoms include disproportionate limb growth, limited joint mobility, difficulty walking, delayed motor development, or abnormal posture (e.g., scoliosis, bowlegs).
Some dysplasias can be detected as early as during pregnancy through prenatal ultrasound. Others are diagnosed in the first few months of a child’s life or later in childhood, when more pronounced abnormalities in bone growth and structure become apparent.
Genetic skeletal dysplasias cannot be completely cured. However, effective symptomatic treatment is possible—correcting deformities, improving motor function, and enhancing the patient’s quality of life. Early diagnosis and comprehensive treatment significantly improve the prognosis.
Treatment is tailored to each individual and may include rehabilitation, physical therapy, orthopedic devices, and surgical intervention. In cases of limb alignment deformities, treatments may include minimally invasive hemiepiphysiodesis or corrective osteotomies.
With early diagnosis and appropriate treatment, many children achieve full or significantly improved mobility. The outcome depends on the type and severity of the dysplasia, as well as when treatment begins.
Surgical treatment is recommended when bone or joint deformities significantly limit limb function, cause pain, or continue to progress despite conservative treatment. The decision is made by an orthopedic surgeon following a detailed imaging evaluation.